What effect will the Court’s abortion ruling have on laws in other states?
on Sep 19, 2016 at 1:40 pm
In June the Court struck down two provisions in a Texas law regulating abortions in that state. One required physicians who perform abortions to have admitting privileges at hospitals less than thirty miles from the abortion clinic, while the other required clinics to have facilities comparable to ambulatory surgical centers.
More than two dozen states have requirements that are at least somewhat similar; some of those requirements either are or recently were also the subject of legal challenges. Most notably, just one day after its ruling in the Texas case, the Court rejected requests by officials in Wisconsin and Mississippi to review lower-court decisions blocking the enforcement of admitting privileges requirements in those states.
Using resources provided by the Center for Reproductive Rights and the Guttmacher Institute, we identified four basic categories of state requirements regarding admitting privileges.
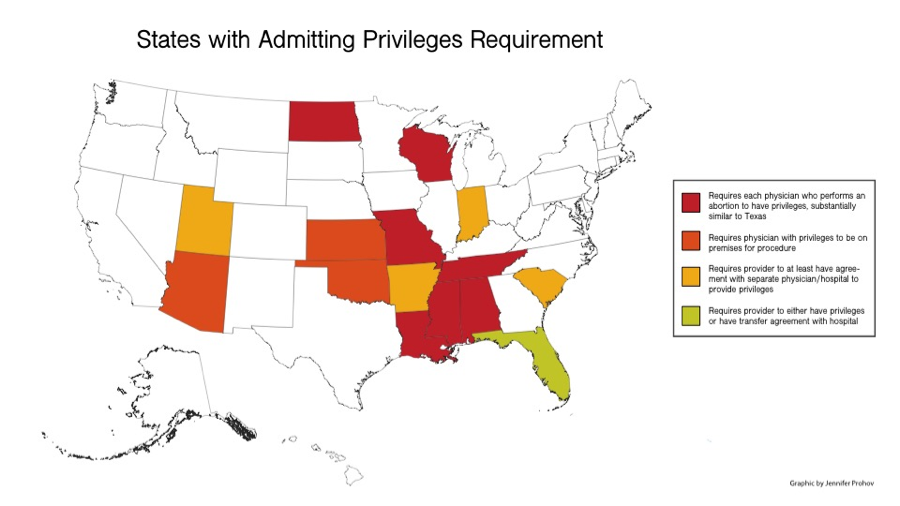
(Click chart to enlarge)
The first category is made up of states with laws and regulations that are substantially similar to Texas’s admitting privileges law, which requires all physicians who perform abortions in the state to have “active admitting privileges” at a hospital within thirty miles of the clinic that provides “obstetrical or gynecological health care services.” In addition to Texas, courts have blocked the enforcement of these requirements in Alabama, Louisiana, Mississippi, and Wisconsin.
- Alabama: All physicians who perform abortions must have “staff privileges at an acute care hospital within the same standard metropolitan statistical area” as the abortion clinic.
- Louisiana: All physicians who perform abortions must “have active admitting privileges at a hospital,” no more than thirty miles away, that provides obstetrical or gynecological services.
- Mississippi: The state’s law is more stringent than its Texas counterpart, requiring all physicians associated with a clinic – rather than just physicians who perform abortions – to “have admitting privileges at a local hospital and staff privileges to replace local hospital on-staff physicians.”
- Missouri: All physicians who perform abortions must have clinical privileges “at a hospital which offers obstetrical or gynecological care located within thirty miles.”
- North Dakota: All physicians who perform abortions “must have admitting privileges at a hospital located within thirty miles” of the clinic and “staff privileges to replace hospital on-staff physicians at that hospital.”
- Tennessee: Physicians who perform abortions must have admitting privileges at a hospital either in the county where the abortion is performed or in an adjacent county.
- Wisconsin: All physicians who perform abortions must have admitting privileges at a hospital no more than thirty miles away.
A second category of state laws and regulations requires clinics to have a physician with admitting privileges at a nearby hospital on the premises whenever abortions are being performed, but the person who actually performs the abortion is not required to have admitting privileges herself. Enforcement of the requirement has been blocked by a court order in Oklahoma. These states are:
- Arizona: A physician with admitting privileges must be on the clinic’s premises while the procedure is performed and must remain there until the patient is stable and ready to leave. For surgical abortions, the physician must have privileges at a hospital no more than thirty miles away by car; the requirement does not specify how close the hospital must be for medical — that is, non-surgical – abortions.
- Oklahoma: State law requires a physician with admitting privileges at a hospital within thirty miles to be on the premises whenever abortions are performed; the physician must stay there until all patients are stable and ready to leave.
A third category of state laws and regulations requires clinics to have either a physician on staff with admitting privileges at a nearby hospital or some form of an agreement with a physician with such privileges to ensure care for their patients if complications occur. Courts have blocked enforcement of these requirements in Arkansas and Kansas.
- Arkansas: All physicians who provide an “abortion-inducing drug” must have a contract with a physician who will handle complications and “has active admitting privileges and gynecological/surgical privileges at a hospital designated to handle any emergencies” arising from the procedure.
- Indiana: Any physician who performs an abortion must have either admitting privileges at a hospital in the same or neighboring county or a written agreement “concerning the management of possible complications” from the abortion with a physician who does have admitting privileges.
- Kansas: A 2011 state law directs the Secretary of Health and Environment to adopt regulations that, at a minimum, require a physician with admitting privileges at a hospital within thirty miles of the clinic to be “available.”
- South Carolina: An abortion clinic must have a physician on staff or contract with one with admitting privileges “at one or more local hospitals with OB/GYN services to ensure his/her availability to the staff and patients during all operating hours.”
- Utah: Every abortion facility in the state must either have a medical director with admitting privileges at a hospital within fifteen minutes or a transfer agreement with a hospital within fifteen minutes that provides hospital admitting privileges for the facility’s medical director or attending physician.
A fourth category of state laws and regulations requires physicians who perform abortions to have admitting privileges at a nearby hospital – unless the clinic has a transfer agreement with a nearby hospital, in which case admitting privileges are not required.
- Florida: Physicians who perform abortions must have admitting privileges “at a hospital within reasonable proximity to the clinic, unless the clinic has a written patient transfer agreement with a hospital within reasonable proximity to the clinic.”
State laws and regulations establishing surgical-center requirements are harder to categorize. Elizabeth Nash, a senior associate at the Guttmacher Institute, explains that, although states may require abortion clinics to meet standards similar to those for surgical centers in that particular state, the substance of those standards can vary significantly. For example, she notes, Maryland’s standards for surgical centers “are very different than what you would find in Texas.”
Clinics also may be subject to different requirements depending on whether they perform both medical and surgical abortions or only one type of abortion.
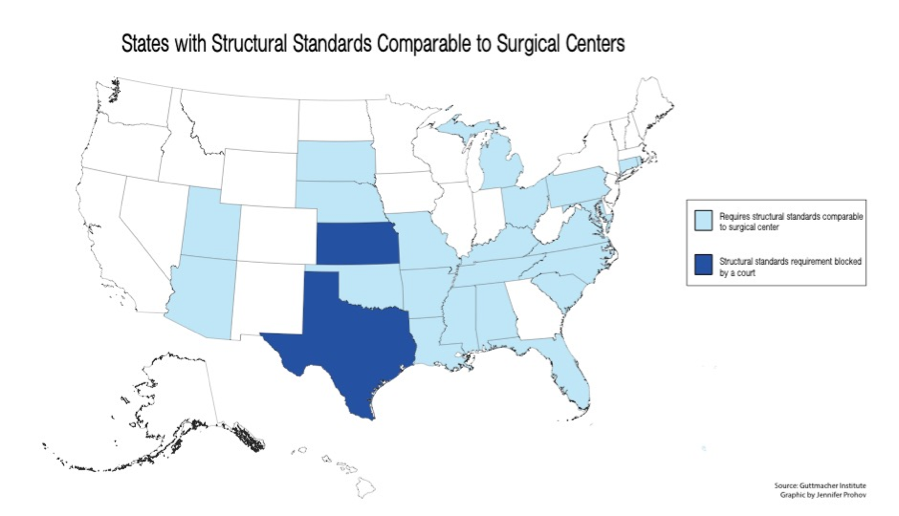
(Click chart to enlarge)
The Guttmacher Institute identifies twenty-three states (in addition to Texas) that require abortion clinics to meet the “structural standards comparable to surgical centers” of the state: Alabama, Arizona, Arkansas, Connecticut, Florida, Kansas (where enforcement of the requirement is currently blocked by court order), Kentucky, Louisiana, Maryland, Michigan, Mississippi, Missouri, Nebraska, North Carolina, Ohio, Oklahoma, Pennsylvania, Rhode Island, South Carolina, South Dakota, Tennessee, Utah, and Virginia.